
Meningioma Information
|
This is a tumour in your meninges. These thin layers of protective tissue surround your brain and spinal cord. Most meningiomas are not cancerous (benign) and usually grow slowly. Meningiomas are the third most common type of brain tumour representing 25% of primary brain tumours.
Meningiomas usually cause symptoms by pressing on a part of the brain next to where they are growing. This can cause a wide range of problems such as headaches, seizures, visual problems or weakness in your arms and legs. Sometimes meningiomas cause no symptoms and are diagnosed during investigations ordered for other reasons. The diagnosis of a meningioma generally requires a scan of the brain, such as a CT or MRI. The options for treating meningiomas include surgery to remove the meningioma, or adopting a watch-and-wait approach. Sometimes treatment with radiotherapy will be recommended. Watch the video below for more information about meningiomas. Read below for more detailed information about meningiomas. |
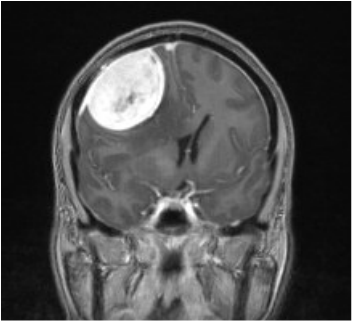
Large right frontal meningioma in a young lady. This tumour was completely removed without any complications.
|
Brain Tumour Video - Meningiomas
What is a meningioma?
A Meningioma is a type of benign brain tumour which grows from the linings of the brain called the meninges. Over 95% of meningiomas are benign tumours. Rarely these tumours can grow more rapidly and show more malignant or aggressive behaviour. Meningiomas are very common brain tumours and represents 25% of all primary intracranial tumours. Meningiomas can also occur in the spine, most commonly in the thoracic region. Meningiomas are commonly found incidentally in the population and many do not need treatment, or surgery.
The mean age of presentation of meningiomas is 60 years of age, however, rarely they can occur in childhood or in young adults They are more common in females. Meningiomas can also grow or manifest during pregnancy because of hormonal influences. Sometimes patients have more than one meningioma.
For most patients there is no specific reason why they have developed a meningioma. It is just “bad luck” that it has grown. There are some rare genetic conditions, such as neurofibromatosis (NF1 and NF2), which predispose patients to developing meningiomas. They are also associated with patient's who have had previous radiation to the brain or head. For the most part, there is no reason why patients develop this type of brain tumour and it is not their fault.
Where do meningiomas arise from?
The brain and spinal cord are contained within a protective coverings called the meninges. Meningiomas grow from the arachnoid layer, or middle layer, of the meninges.
The natural history of meningiomas is that they grow very slowly and they typically do not infiltrate into the brain. This is why, for the most part, they are benign. Meningiomas can, however, cause pressure on the brain causing symptoms. They can arise in any area of the brain where there is meninges or dura.
Common locations for meningiomas include parasagittal region, convexity, sellar region, sphenoid wing, olfactory groove and CP angle/posterior fossa. Rarely these tumours can occur within the ventricles.
Classification of Meningiomas:
Meningiomas are typically classified into grades I, II or III. Grade I tumours represent 95% of tumours and are benign tumours. There are many subtypes of grade I meningiomas.
5% of tumours have propensity for increased or more rapid growth. These types of tumours are described as grade II meningiomas (atypical) or grade III meningomas (anaplastic).
The exact type of meningioma can only be accurately determined once the tumour is removed and analysed by a pathologist.
Clinical Presentation of Meningiomas:
Meningiomas can present in a variety of different ways. The common symptoms include:
1. Seizures
2. Found incidentally or asymptomatic during a brain scan performed for another reason
3. Headaches
4. Focal neurological deficits such as weakness, numbness or speech disturbance
5. Raised intracranial pressure including headache, nausea and vomiting
6. Cranial nerve compression causing symptoms such as visual problems, deafness or facial numbness
7. Balance disturbance or dizziness
The exact presentation depends on the location of the meningioma and its size. A lot of the above symptoms are non-specific and most patients exhibiting the above symptoms of headache, dizziness or nausea will not have a brain tumour.
Investigations for meningiomas:
Most meningiomas will show up on a contrast enhanced CT scan. There may be areas of calcification within the tumpour on CT. Small meningiomas may be difficult to see on a CT scan of the brain.
The gold standard for diagnosis is an MRI scan of the brain with contrast. This will show an enhancing lesion on the surface of the brain. Meningiomas have a fairly classic appearance including being extra-axial and having a dural tail.
Treatment of meningiomas:
The treatment options for meingiomas include:
Surgery for meningiomas:
For tumours that are large, are causing symptoms or show signs of growth, surgery is usually required. The goal of surgery is to remove the tumour safely without causing harm to the patient. Given these tumours are generally benign sometimes it is safer to remove only part of the tumour. The exact surgical procedure depends on the location of the meningioma. Usually the procedure would involve a craniotomy to remove the tumour with excision of the dural attachment. See our surgery for meningiomas page for more information or watch the video below.
A Meningioma is a type of benign brain tumour which grows from the linings of the brain called the meninges. Over 95% of meningiomas are benign tumours. Rarely these tumours can grow more rapidly and show more malignant or aggressive behaviour. Meningiomas are very common brain tumours and represents 25% of all primary intracranial tumours. Meningiomas can also occur in the spine, most commonly in the thoracic region. Meningiomas are commonly found incidentally in the population and many do not need treatment, or surgery.
The mean age of presentation of meningiomas is 60 years of age, however, rarely they can occur in childhood or in young adults They are more common in females. Meningiomas can also grow or manifest during pregnancy because of hormonal influences. Sometimes patients have more than one meningioma.
For most patients there is no specific reason why they have developed a meningioma. It is just “bad luck” that it has grown. There are some rare genetic conditions, such as neurofibromatosis (NF1 and NF2), which predispose patients to developing meningiomas. They are also associated with patient's who have had previous radiation to the brain or head. For the most part, there is no reason why patients develop this type of brain tumour and it is not their fault.
Where do meningiomas arise from?
The brain and spinal cord are contained within a protective coverings called the meninges. Meningiomas grow from the arachnoid layer, or middle layer, of the meninges.
The natural history of meningiomas is that they grow very slowly and they typically do not infiltrate into the brain. This is why, for the most part, they are benign. Meningiomas can, however, cause pressure on the brain causing symptoms. They can arise in any area of the brain where there is meninges or dura.
Common locations for meningiomas include parasagittal region, convexity, sellar region, sphenoid wing, olfactory groove and CP angle/posterior fossa. Rarely these tumours can occur within the ventricles.
Classification of Meningiomas:
Meningiomas are typically classified into grades I, II or III. Grade I tumours represent 95% of tumours and are benign tumours. There are many subtypes of grade I meningiomas.
5% of tumours have propensity for increased or more rapid growth. These types of tumours are described as grade II meningiomas (atypical) or grade III meningomas (anaplastic).
The exact type of meningioma can only be accurately determined once the tumour is removed and analysed by a pathologist.
Clinical Presentation of Meningiomas:
Meningiomas can present in a variety of different ways. The common symptoms include:
1. Seizures
2. Found incidentally or asymptomatic during a brain scan performed for another reason
3. Headaches
4. Focal neurological deficits such as weakness, numbness or speech disturbance
5. Raised intracranial pressure including headache, nausea and vomiting
6. Cranial nerve compression causing symptoms such as visual problems, deafness or facial numbness
7. Balance disturbance or dizziness
The exact presentation depends on the location of the meningioma and its size. A lot of the above symptoms are non-specific and most patients exhibiting the above symptoms of headache, dizziness or nausea will not have a brain tumour.
Investigations for meningiomas:
Most meningiomas will show up on a contrast enhanced CT scan. There may be areas of calcification within the tumpour on CT. Small meningiomas may be difficult to see on a CT scan of the brain.
The gold standard for diagnosis is an MRI scan of the brain with contrast. This will show an enhancing lesion on the surface of the brain. Meningiomas have a fairly classic appearance including being extra-axial and having a dural tail.
Treatment of meningiomas:
The treatment options for meingiomas include:
- Observation: Small meningiomas which have imaging characteristics of a classic of meningioma can be watched with serial scans of the brain over time. If they do not demonstrate growth and remain asymptomatic then often these tumours are able to be left alone without surgery. Should these tumours change or have atypical features then surgery to remove the tumour may be indicated. Dr Oehme will advise if it is safe to watch a meningioma or whether surgery is a better treatment option.
- Surgery to remove the tumour
- Radiotherapy or stereotactic radiosurgery
Surgery for meningiomas:
For tumours that are large, are causing symptoms or show signs of growth, surgery is usually required. The goal of surgery is to remove the tumour safely without causing harm to the patient. Given these tumours are generally benign sometimes it is safer to remove only part of the tumour. The exact surgical procedure depends on the location of the meningioma. Usually the procedure would involve a craniotomy to remove the tumour with excision of the dural attachment. See our surgery for meningiomas page for more information or watch the video below.
Craniotomy (Surgery) For Meningioma
This procedure, performed under general anesthesia, creates an opening through the skull for removal of a meningioma. This type of tumor is found in the dura - the fibrous membrane between the brain and skull. The surgery usually requires several hours to complete, depending on the location and size of the meningioma.
Following removal you will be monitored with yearly scans to ensure that the tumour does not grow back, or to keep an eye on any tumour that was left behind at the initial operation.
Recurrence of meningiomas
Sometimes meningiomas can grow back following removal. This is known as recurrence. Recurrence of meningiomas depends on the type of meningioma and the amount removed. Generally, if they do recur, they do so in a very slow fashion. Tumours that are completely removed have a very low chance of recurrence, generally less than 10%.
Other treatments for meningiomas:
Other treatment options for tumours that recur following surgery or cannot be safely removed include:
1. Further surgery
2. Radiation treatment. This can include stereotactic radiosurgery.
3. Rarely chemotherapy.
Dr Oehme will explain your treatment options for your meningioma at your consultation.